Head Injury
Head Shaking or Trauma: Don’t Ignore Even Minor Head Injuries
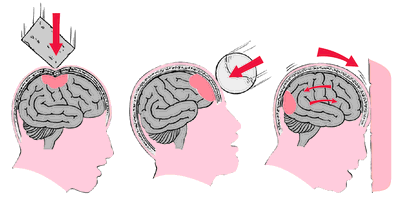
Bumping your head accidentally on a cabinet, a playful shove, or any incident causing head shaking or injury is extremely common—and often overlooked or forgotten. Many patients only notice discomfort 3 weeks to 3 months later and then seek help from a neurosurgeon. Only after examination does the doctor discover signs of prior head impact or trauma.
In clinical analysis of over 200 traumatic brain injury (TBI) patients, half had no memory of any head shaking or trauma event. Head shaking or impacts happen frequently in daily life. They range from minor scalp injuries to severe cases causing loss of consciousness and life-threatening risks.
Even in car accidents or falls where you hit your head, don’t assume no bleeding or visible external wound means no need for medical check-up. A common clinical scenario is intracranial hemorrhage (brain bleeding) with no external wound at all.
If your head has experienced shaking or impact, both the patient and family must watch closely for these key warning signs:
- Brief loss of consciousness or partial amnesia at the time of injury.
- Monitor if the person’s consciousness remains clear—observe continuously for at least 3 days.
- Worsening headache and vomiting (getting progressively more severe).
- Numbness or weakness on one side of the body (arms or legs).
- Unsteady gait or balance issues—possible cerebellar injury.
- For traumatic brain injury patients, family members should closely monitor during sleep at night: wake the person periodically to confirm they are arousable and not becoming drowsy or comatose due to intracranial bleeding pressing on the brain.
Classification of Head Trauma Severity – Glasgow Coma Scale (GCS)
The Glasgow Coma Scale (GCS) is a standard tool to assess level of consciousness. It scores out of 15 (best) to 3 (worst), based on three components: Eye opening (E), Motor response (M), and Verbal response (V). The total is the GCS score.
Within the first 20 minutes after head trauma, GCS classification includes:
- (A) Mild head injury: GCS 13–15
- (B) Moderate head injury: GCS 9–12
- (C) Severe head injury: GCS 8 or below
Head Trauma Examination and Management
CT scan (computed tomography) and MRI are widely used today. CT is especially valuable in the acute phase, clearly showing intracranial hematomas, brain contusions, edema, and other injuries. For head trauma patients who are unconscious, have neurological deficits, or suspected intracranial hematoma, arrange urgent CT scan (in addition to skull X-ray when needed).
Common Types of Head Injuries, Symptoms, and Complications
Scalp hematoma: After impact, often swells like an egg and is very painful. Treatment: No ointment, no rubbing, no hot compress—usually resolves in about 1.5 months.
Scalp laceration: Focus on stopping bleeding and keeping the wound clean.
Headache after head injury: Varies greatly—mild to unbearable, constant or episodic, dull, throbbing, burning, or pressure-like. Can be diffuse (whole head) or localized. Often worsens with posture change, stress, fatigue, or straining; improves with rest or simple painkillers.
Dizziness: Usually intermittent, lasting minutes each time. Triggered by posture change or stress; improves when lying down with eyes closed. About half of mild head injury patients experience dizziness, with half lasting over 2 months. Roughly 75% of dizzy patients also have headache, and vice versa.
Concussion (mild traumatic brain injury): Even without visible head wound, a strong blow can cause brief loss of consciousness, hearing/smell issues, short-term memory loss, headache, dizziness, confusion, blurred vision, unsteady gait, tinnitus, nausea, insomnia, poor concentration, emotional changes, or lack of motivation. Never ignore this—seek a neurosurgeon promptly. Proper management prevents permanent sequelae.
Brain contusion/traumatic brain injury: Direct brain tissue damage at impact site, often with intracranial bleeding. Beyond concussion symptoms, severe cases cause drowsiness, coma, seizures, limb weakness, abnormal behavior/personality changes, rapid breathing, etc.
Intracranial hemorrhage (brain bleed): Blood clot directly compresses brain tissue, causing headache, vomiting, rapid breathing, facial/limb seizures, dizziness, limb weakness/numbness, altered consciousness, drowsiness, or coma. Seek immediate medical help—untreated can lead to permanent disability or death. The most lethal complication in head trauma is subdural or epidural hematoma.
- Chronic subdural hematoma: Common in elderly (>50) or young children. Often from minor falls (e.g., getting up at night to use the bathroom, unsteady walking). Symptoms appear slowly 2 weeks or more after injury (even up to 2 years). Includes headache, one-sided weakness (stroke-like), memory decline, poor appetite, bilateral leg weakness, unsteady gait (cerebellar involvement). Electrolyte imbalance can mimic weakness, delaying diagnosis. Incidence is low (1–3%). Brain often absorbs small bleeds naturally, but large or prolonged pressure on brainstem requires prompt minimally invasive burr hole drainage to relieve pressure—otherwise risks respiratory failure, permanent disability, or death.
- Epidural (extradural) hematoma: From torn intracranial vessel after impact. The dura is the tough outer protective layer. If bleeding is not massive, severe unusual headache may appear days 4–5 after injury (average timing). Some are misdiagnosed as migraine or tension headache. Always inform your doctor of any prior head trauma for accurate differential diagnosis.
Brain laceration with skull fragments: Direct tissue damage; symptoms similar to contusion or hemorrhage.
Brain edema (swelling): Injured brain cells swell, worsening central nervous system damage and possibly causing hemorrhage.
Brain ischemia: Raised intracranial pressure reduces blood supply, leading to cell damage or death.
Post-traumatic epilepsy: 2–7% of brain trauma patients develop seizures (higher in moderate/severe cases). Monitor EEG for abnormalities; severe cases require anti-epileptic medication.

Important Precautions After Head Trauma
The first 72 hours post-injury are critical for observation. If any of these appear, contact a neurosurgeon immediately or go to the hospital for further evaluation:
- Brief loss of consciousness or amnesia at injury time
- Severe or worsening headache/dizziness
- Excessive drowsiness or inability to wake up (progressive loss of consciousness)
- Apathy, poor concentration, or personality changes
- Disorientation to time or place
- Nausea, vomiting, vertigo
- One-sided numbness or weakness in limbs
- Unsteady walking or gait
- During sleep, family should wake the patient periodically to check alertness—prevent delayed coma from brain bleed pressing on vital structures
Early recognition and prompt medical attention can prevent serious complications from head injuries, concussions, or traumatic brain injury. If in doubt, always seek professional evaluation.

